
Functional Neurological Disorder (FND) is a common neurological condition — yet many people have never even heard of it. Even more concerning, it is still widely misunderstood.
I was reminded of this when I recently attended a conference at the Walton Centre, a specialist neurology and neurosurgery trust in the North West. During the conference, consultant neurologist Dr Christine Burness gave a talk on FND that shifted my perspective on how we understand and approach the condition.
As a doctor, FND has always been on my radar. But Dr Burness’s talk challenged some of my assumptions and prompted me to think more carefully about how we assess and explain neurological symptoms that don’t fit traditional patterns. It highlighted how easily FND can be misunderstood — not only by patients, but by healthcare professionals also. If her talk could change my perspective, I hope this article might shift yours too.
So let’s start with the basics.
Contents
- What is FND?
- What causes FND?
- FND symptoms
- How is FND diagnosed?
- FND management
- FND prognosis
- Misconceptions and stigma
- In summary
DISCLAIMER:
While I am a practising doctor, the information on this site is for educational purposes only. It does not take into account your personal circumstances, which can significantly affect medical decision-making and treatment. This content therefore does not constitute medical advice, and should not be relied upon for diagnosis or treatment. Always consult a qualified healthcare provider regarding any health concerns.
This article was published on the 09/03/2026 using up-to-date sources at that time. Please be aware that medical information and guidelines change often.
What is FND?
Functional Neurological Disorder is defined by the National Institute for Health and Care Excellence (NICE) as:
“A condition in which a person experiences neurological symptoms caused by a disorder of nervous system functioning, rather than a structural neurological disease.”
At the point of diagnosis, these symptoms are causing significant distress or impairment in quality of life. When similar symptoms are present but milder or less disabling, they may be referred to more broadly as functional neurological symptoms.
Historically, the diagnosis has been surrounded by skepticism. However, the absence of a structural abnormality does not mean the condition is any less real or disabling.
And unfortunately, this misunderstanding can occur among both clinicians and patients. Part of the problem may lie in the name itself: the word “functional” can carry negative connotations and is sometimes wrongly interpreted as meaning “not real” or “psychological.”
What causes FND?
The exact cause of FND is not fully understood. However, our understanding of the condition has changed significantly in recent years.
FND was often thought to arise from psychological distress/emotional trauma. The condition used to be referred to as conversion disorder, reflecting the belief that psychological distress was “converted” into physical neurological symptoms. While psychological distress can play a role, modern research has shown that this explanation alone is too simplistic.

Research using advanced brain imaging techniques has demonstrated that FND involves changes in the way brain networks communicate with one another. For this reason, many researchers now describe FND as a “brain network disorder.”
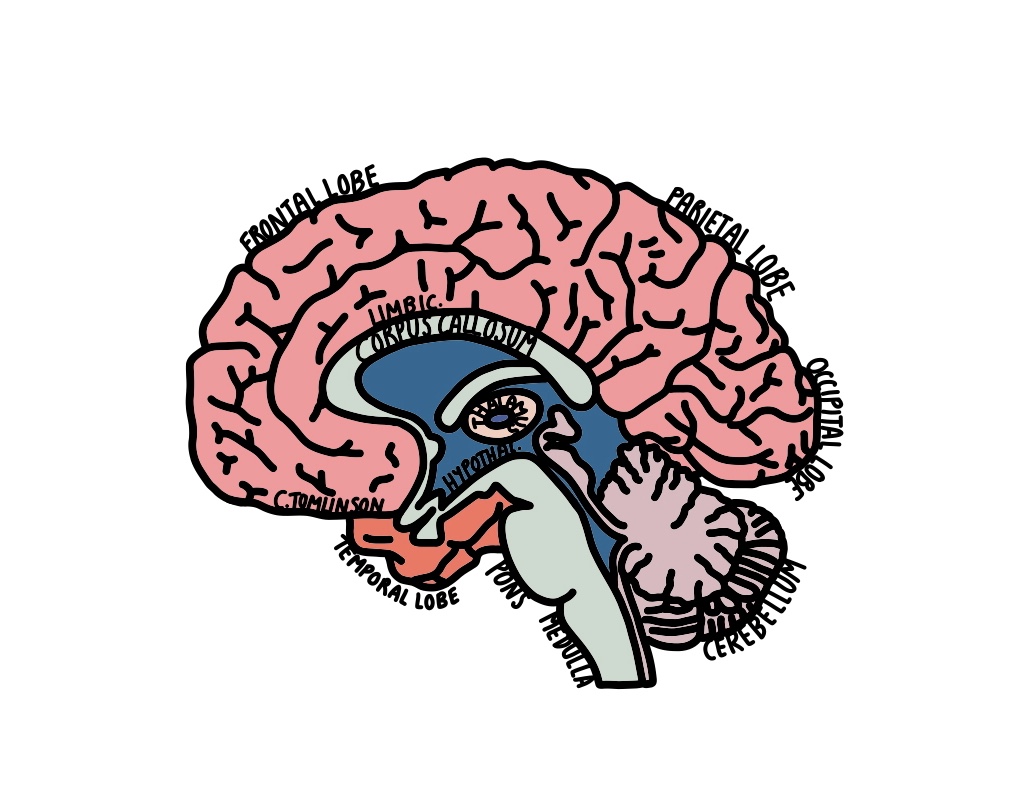
Studies using functional brain imaging (such as fMRI) have identified altered activity in several areas of the brain involved in movement, emotion, attention, and self-awareness. These include regions such as the amygdala, insular cortex, and temporoparietal junction.
These findings suggest that in FND, the brain is capable of generating normal movement and sensation, but the systems that coordinate and control these functions are not working together in the usual way.
The brain and predictive processing
One way scientists explain FND is through the idea that the brain is constantly predicting what it expects to happen; it is a “predictive” organ.
In FND, these prediction systems may become disrupted. The brain may generate incorrect predictions about movement or sensation, which can interfere with normal control of the body.
For example, the brain might send signals to move a limb, but the expected feedback from that movement does not match the brain’s prediction. This mismatch can lead to symptoms such as tremor, weakness, or abnormal movement patterns.
Risk factors and triggers
FND can sometimes begin after a triggering event, but this varies widely between individuals.
Triggers can include a physical illness or injury, psychological stress, or other traumatic experiences. Having an existing neurological condition also increases the risk of developing FND.

Research shows that a history of trauma is more common in people with FND — one study suggests it may be up to eight times more frequent than in the general population. However, many people with FND do not have any identifiable trigger, which suggests that genetic or other biological factors may also play a role.
FND symptoms
FND can present in many different ways, and not everyone will experience all of these symptoms. Many people have a combination of several symptoms, which may change over time:
Motor (movement) symptoms
| Symptom | What it means / What someone might experience |
|---|---|
| Tremor | Involuntary rhythmic shaking of a body part. A hand, arm, or leg may shake. It may worsen when someone is stressed, tired, anxious, after caffeine, or in very hot or cold environments. |
| Dystonia | Involuntary muscle contractions that cause abnormal postures or twisting movements. Examples include a hand clenching into a fist, the neck twisting to one side, or uncontrolled blinking. These movements can sometimes be painful. |
| Jerks or tics | Sudden, brief, involuntary movements or sounds. This may include shoulder jerks, head movements, or vocal sounds that are difficult to control. |
| Weakness | Reduced ability to move or control part of the body. An arm or leg may feel heavy, weak, or difficult to move, and symptoms may fluctuate throughout the day. |
Sensory symptoms
| Symptom | What it means / What someone might experience |
|---|---|
| Tingling (“pins and needles”) | An abnormal sensation often described as prickling, buzzing, or electric. A limb may feel like it is “asleep” even without pressure or injury. |
| Numbness | Reduced or absent sensation in part of the body. Someone may find it difficult to feel touch, temperature, or pain in an area of skin. |
| Tinnitus | Hearing sounds without an external source. This is often described as ringing, buzzing, or humming in the ears. Some people hear their heartbeat. |
| Vision or hearing loss | Partial or complete loss of sight or hearing without structural damage to the eyes or ears. This may appear suddenly or fluctuate. |
Walking and balance
| Symptom | What it means / What someone might experience |
|---|---|
| Gait disturbance | Changes in the way someone walks. Walking may become slow, hesitant, or unsteady, and legs may feel difficult to control or occasionally buckle. |
Dizziness
| Symptom | What it means / What someone might experience |
|---|---|
| Persistent postural–perceptual dizziness (PPPD) | A chronic sense of dizziness or unsteadiness that is usually worse when standing upright, moving, or in visually busy environments such as supermarkets or crowds. |
Cognitive symptoms
| Symptom | What it means / What someone might experience |
|---|---|
| Memory problems | Difficulty recalling information or recent events, such as forgetting conversations, appointments, or where items were placed. |
| Word-finding difficulty | Knowing what you want to say but struggling to retrieve the word. People may pause, hesitate, or substitute vague words like “thingy.” |
| Concentration difficulties | Reduced ability to focus or sustain attention. This may include losing track of conversations, rereading the same sentence, or struggling to complete tasks. |
Seizure-like episodes
| Symptom | What it means / What someone might experience |
|---|---|
| Functional (dissociative) seizures | Episodes that resemble epileptic seizures but are not caused by abnormal electrical activity in the brain. They may involve shaking, altered awareness, or unusual movements such as pelvic thrusting or side-to-side head movements. Episodes can vary in duration and intensity. |
How is FND diagnosed?
One important thing to note is that FND shouldn’t be a diagnosis of exclusion (i.e., a diagnosis that is made after everything else has been ruled out). Instead, clinicians make a “rule-in” diagnosis by identifying positive clinical signs that are characteristic of FND.
There are a few general key features of FND symptoms:
- Internal inconsistency
- Symptoms may change depending on the situation or the task being performed. For example, weakness might appear during formal strength testing but improve during other movements.
- Improvement with distraction
- Abnormal movements such as tremor may lessen or disappear when attention is directed toward another task.
- Symptoms don’t match typical neuroanatomy
- Sensory changes or weakness may not follow patterns expected from nerve injury or damage to a specific part of the brain.
When a diagnosis of FND is suspected, patients are usually referred to a neurologist for special assessment.
It is important to note that, particularly in patients with a pre-existing diagnosis of FND, any new neurological symptoms should be reassessed urgently to exclude an alternate diagnosis.
FND management
Primary and Secondary Care
For many people with FND, care begins at the primary care level (GP) or in secondary care such as hospitals or community clinics. These services provide a clear diagnosis, explain the condition, and offer guidance on self-management. They can also provide access to therapies including physiotherapy, occupational therapy, neuropsychology, and speech and language therapy.

Specialist services
When symptoms are persistent, severe, or the diagnosis is unclear, patients may be referred to regional neuroscience centres for specialist input. These centres provide multidisciplinary (MDT) care, advanced diagnostic testing, and targeted interventions for specific symptom types, such as functional seizures or fixed dystonia.
Key therapies and other support
- Neuropsychiatry and neuropsychology support cognition, stress management, and tailored therapies such as cognitive-behavioural therapy (CBT).
- Neuro-Physiotherapy focuses on retraining movement and motor control.
- Occupational therapy helps with daily activities, energy conservation, and returning to work or education.
- Speech and language therapy (SALT) can improve functional speech, voice, or swallowing.
- Pain management and social care support help address co-existing pain, daily living challenges, and maintaining independence.

Self-management strategies
Patients often benefit from practical strategies to manage symptoms day-to-day. These include grounding techniques, relaxation exercises, maintaining consistent sleep and rest, tracking activity and symptoms, and pacing to balance low-energy activities with recovery periods.
Peer and charity support (UK)
Charities such as FND Action, FND Hope, and The Brain Charity offer resources, support groups, webinars, and guidance for patients and families, providing connection, practical advice, and encouragement alongside professional care.
FND prognosis
The long-term outlook for FND varies widely. Many people experience fluctuating symptoms that can come and go, and some develop new symptoms over time. Studies suggest that complete remission is relatively uncommon, with only around 20–33% of patients fully recovering, though current evidence remains limited. People with FND often have similar levels of disability and impacts on quality of life as those with other neurological conditions, such as epilepsy or multiple sclerosis.
Overall, NICE reports that people with FND tend to experience poorer long-term physical health, which is partly due to under-diagnosis, limited understanding and acceptance of the condition, and the lack of specialist FND services across the UK. Early diagnosis and access to supportive, multidisciplinary care can make a meaningful difference in outcomes and quality of life.
Misconceptions and stigma
FND is often misunderstood, even among healthcare professionals. Dr Christine Burness gave an example of a fictional patient whose tremor worsened during a morning ward round, when they were focused on their symptoms, but seemingly improved or disappeared when asked if they wanted a cup of tea as the trolley came by. To someone unfamiliar with FND, this might look like the patient was “putting on symptoms.” In reality, this is a classic feature of FND: symptoms can fluctuate with attention or distraction and are not under the person’s conscious control.
FND is a genuine, disabling condition caused by changes in brain networks, not intentional behaviour. We all have a responsibility to talk about FND and help raise awareness, so that people feel supported, and understood.
In summary
FND is a genuine, often misunderstood condition that causes significant disruption to the functioning of the nervous system, in turn affecting daily life. Symptoms can fluctuate, and recovery varies, but early diagnosis and access to MDT care can improve outcomes. Understanding, empathy, and practical support — from healthcare professionals, peer networks, and charities — are essential for helping people with FND live well. Raising awareness and challenging stigma is a responsibility we all share.
- What did you learn from this article about FND, and did anything surprise you?
- Are there any other myths or misconceptions about FND that you’ve encountered before reading this?
- If you or someone you know have FND, are there any other strategies that help manage it?
I’d love to hear from you! Please leave a comment down below.

Leave a comment