
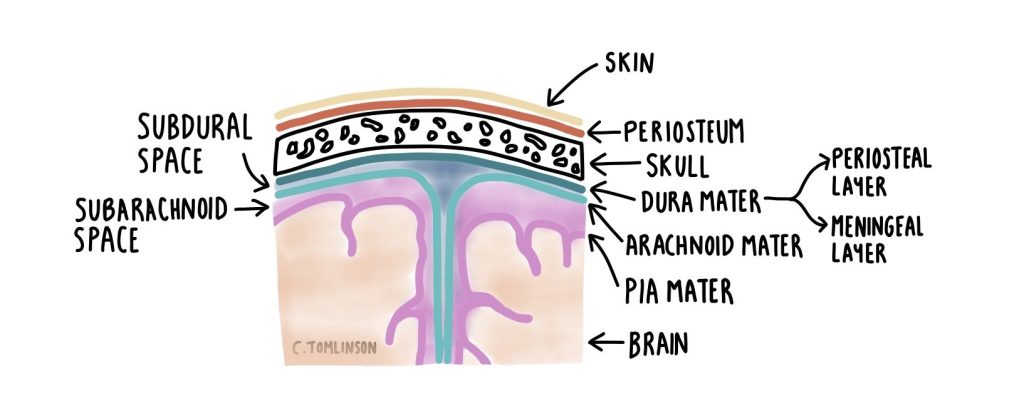
Meningitis is an inflammation of the meninges, the protective layer that surrounds the brain and spinal cord, made up of dura mater, arachnoid mater, and pia mater (see below). It can be caused by a number of infective and non-infective factors.
The recent Kent 2026 MenB outbreak has brought meningitis back into the spotlight, with many people contacting their GP or NHS 111 to ask what it is and whether they might be at risk — something I’ve noticed myself this week, too — as people are understandably concerned. While relatively rare, meningitis can progress rapidly and cause serious complications if not recognised and treated promptly.
So what exactly is meningitis? How is it treated, and what can be done to prevent it? Let’s find out.
Contents
- What causes meningitis
- Kent meningitis outbreak 2026
- How meningitis spreads
- Early signs of meningitis
- Meningitis signs and symptoms
- When to seek help
- Diagnosis of meningitis
- Meningitis treatment
- Meningitis complications
- Meningitis vaccination
- Meningitis prevention
- In summary
DISCLAIMER:
While I am a practising doctor, the information on this site is for educational purposes only. It does not take into account your personal circumstances, which can significantly affect medical decision-making and treatment. This content therefore does not constitute medical advice, and should not be relied upon for diagnosis or treatment. Always consult a qualified healthcare provider regarding any health concerns.
This article was published on the 30/03/2026 using up-to-date sources at that time. Please be aware that medical information and guidelines change often.
What causes meningitis
Meningitis can be due to viral, bacterial, fungal, or parasitic infections, with viral causes being the most common. Bacterial meningitis tends to be the most serious type of meningitis, with there being four main commonly implicated bacteria:
- Neisseria meningitidis (meningococcus)
- Streptococcus pneumoniae (pneumococcus)
- Haemophilus influenzae
- Streptococcus agalactiae (group B streptococcus).
Viral meningitis tends to be less severe than bacterial. The most common viral cause is enteroviruses e.g., Coxsackie virus; other causes include Herpes Simplex, Human Immunodeficiency Virus (HIV), and Varicella-Zoster.
Fungal meningitis typically occurs in people who are immunosuppressed, such as those with Human Immunodeficiency Virus (HIV). Cryptococcus neoformans is an example of this; it is a significant cause of HIV-associated mortality in places with limited access to anti-retroviral treatment (ART).
Non-infective causes of meningitis include cancer, autoimmune conditions e.g., lupus, head injury, certain medications e.g., the antibiotic co-trimoxazole, or surgery e.g., spinal surgery. These are typically more rare.
Kent meningitis outbreak 2026
In March 2026, there was a sudden rise in the number of meningitis cases in Kent, particularly amongst students. As of the 26th of March, there were 20 confirmed cases, and some of the cases have been traced back to nightclub Club Chemistry in Canterbury between the 5th and 7th of March.
The Kent meningitis outbreak 2026 was due to the bacterium Neisseria meningitidis (or meningococcus), in particular the MenB strain. There are lots of different types of meningococcus bacteria: MenA, MenB, MenC, MenW, MenX and MenY.
Since 2015, MenB vaccinations have been available free on the NHS as part of routine childhood vaccinations. Anyone aged over 10 will not have had this vaccine.
Public health authorities launched an investigation into the outbreak and began contact tracing to identify people who may have been exposed. As a precautionary measure, preventative (prophylactic) antibiotics were offered to several groups, including individuals who attended Club Chemistry on 5-7th of March, staff working at the venue, students and staff living on the University of Kent campus, and close household contacts of confirmed cases. Temporary clinics were set up locally to distribute antibiotics to those eligible.
In addition, a small targeted MenB vaccination campaign was introduced for Canterbury Campus Halls of Residence at the University of Kent, in an effort to limit further spread of the infection. This vaccination programme may be expanded in the future to include more people at higher risk, though priority at the moment is with preventing the spread of disease.
How meningitis spreads
How meningitis spreads (transmission) depends on the underlying infective cause, For bacterial meningitis, like MenB, it is usually spread through droplets or secretions from the upper airways. This can include being in close proximity to someone for a prolonged amount of time (as it can spread through droplets in the air they breathe out), or coming into contact with a person’s saliva, such as through kissing or sharing drinks.
Some people can carry meningococcal bacteria in the back of their nose or throat without becoming ill themselves. These individuals are known as carriers, and they can still pass the bacteria to others. In most cases, carrying the bacteria won’t cause any harm to the individual.
Transmission is more likely in situations where people are in close contact for extended periods, such as in student accommodation, shared housing, or crowded social settings.
Early signs of meningitis
Early signs and symptoms tend to be similar to that of the flu or a cold. You may feel headachey, have muscle aches and pains, and a fever.
Meningitis signs and symptoms
Most cases of meningitis present with at least two of: headache, fever, neck stiffness, and altered mental status (i.e., confusion). Other signs/symptoms can include:
- Signs (what can be seen objectively)
- Tachycardia (raised heart rate)
- Hypotension (low blood pressure)
- Non-blanching rash due to “leaky” blood vessels, indicating meningococcal infection
- Seizures
- Symptoms (what the person experiences)
When to seek help
Meningitis can become serious very quickly, particularly if it is caused by bacteria, so it is important to seek medical attention if meningitis is suspected. Anyone experiencing symptoms such as a high fever, severe headache, neck stiffness, confusion, photophobia, persistent vomiting, seizures, or a non-blanching rash should seek urgent medical care. The presence of a non-blanching rash (a rash that does not fade when pressed, sometimes checked using the “glass” or “tumbler” test) may indicate meningococcal infection and requires immediate medical assessment.
In the UK, you should contact NHS 111 for urgent medical advice, or call 999 or go to A&E immediately if symptoms are severe or rapidly worsening. Early diagnosis and treatment are important, as prompt treatment can significantly improve outcomes.
Diagnosis of meningitis
Doctors will first assess a patient’s symptoms and perform a physical examination, looking for signs such as neck stiffness, fever, altered mental state, or a rash. As meningitis can potentially be life-threatening, treatment is often started whilst awaiting further tests if there is clinical suspicion.
The most important test used to confirm meningitis is a lumbar puncture (spinal tap). In this procedure, a small sample of cerebrospinal fluid (CSF) is taken from the lower back using a needle. The CSF can then be analysed in the laboratory to look for signs of infection, including increased white blood cells, changes in glucose and protein levels, and the presence of bacteria or viruses. Laboratory tests such as microscopy, culture, and polymerase chain reaction (PCR) may be used to identify the specific organism responsible. It can be difficult to find the causative organism though in patents where antibiotics have already been given.
Blood tests are also commonly performed. Blood cultures can sometimes identify the bacteria causing meningitis, particularly in cases of bacterial meningitis.
In some situations, brain imaging such as a CT or MRI scan may be performed before a lumbar puncture to check for raised intracranial pressure (ICP). Raised ICP can occur if swelling or fluid accumulation in the brain increases pressure inside the skull. Performing a lumbar puncture in the presence of significantly raised ICP carries a small but serious risk of brain herniation, where brain tissue can be pushed downwards through openings in the skull. Although this complication is rare, imaging helps identify patients at higher risk so that lumbar puncture can be performed safely or temporarily delayed while other treatments, such as intravenous antibiotics or measures to reduce pressure, are given.
Meningitis treatment
Bacterial meningitis is treated with intravenous antibiotics (“through a drip”), often started as soon as meningitis is suspected, even before the specific bacteria is identified. The common first-line antibiotic in the UK is ceftriaxone, though this may vary depending on local guidelines. In some cases, dexamethasone, a steroid, may be given to reduce inflammation in the brain and prevent complications such as hearing loss.
If meningococcal disease is suspected, for example in a patient with a non-blanching rash, paramedics or GPs may give a stat (immediate, one-off) dose of the antibiotics benzylpenicillin or ceftriaxone before hospital transfer, as long as it does not delay urgent transfer to A&E. Similarly, if bacterial meningitis is suspected and there is likely to be a delay in attending hospital, early antibiotics may be administered in the community to reduce the risk of complications.
Viral meningitis is usually less severe and often resolves without specific antiviral treatment. Certain viral infections, such as those caused by herpes simplex virus, may be treated with antiviral medications like aciclovir. Antibiotics will not work on a viral infection.
Fungal and parasitic meningitis are treated with antifungal or antiparasitic medications, depending on the specific cause. For example, fungal meningitis caused by Cryptococcus neoformans is often treated with amphotericin B and flucytosine, while parasitic infections may be treated with drugs such as albendazole.
Treatment of non-infective meningitis focuses on addressing the underlying cause rather than infection. For example, meningitis caused by an autoimmune condition may be treated with immunosuppressive medications, while drug-induced meningitis is managed by stopping the offending medication.
Across all types of meningitis, supportive care is essential. This may include fluids, pain relief, management of fever, and monitoring for complications such as seizures, low blood pressure, or altered consciousness. Patients are typically admitted to hospital for close monitoring.
Meningitis complications
Meningitis can lead to serious complications, particularly if bacterial and not treated early. Potential complications include:
- Hearing loss – one of the most common long-term effects, especially in children.
- Neurological damage – including seizures, learning difficulties, muscle weakness, or memory problems.
- Limb loss (peripheral gangrene) – in severe meningococcal sepsis, poor blood flow can lead to tissue damage and, rarely, amputation.
- Hydrocephalus – a build-up of fluid in the brain.
- Sepsis or shock – life-threatening widespread infection that can cause organ failure.
- Waterhouse-Friderichsen syndrome – a rare but severe complication of meningococcal infection, involving adrenal gland failure (Addison’s disease) due to bilateral adrenal gland haemorrhage.
- Coma or death – in the most severe cases, meningitis can be fatal if not treated urgently.
Meningitis vaccination
Vaccination is the most effective way to prevent meningococcal disease and other forms of meningitis. In the UK, several vaccines are available, depending on age and risk factors:
- MenB vaccine (4CMenB, known as Bexero) – part of the routine childhood immunisation schedule since 2015.
- Since August 2025, it has also been given to gay, bisexual, and men who have sex with men (GBMSM) as it offers cross-protection against Neisseria gonorrhoea (the bacterium that causes gonorrhoea), as Neisseria gonorrhoea is genetically quite similar to Neisseria meningitidis.
- MenACWY vaccine – offered to teenagers and new university students to protect against MenA, MenC, MenW, and MenY strains.
- Pneumococcal vaccine – protects against meningitis caused by Streptococcus pneumoniae, given as part of the routine childhood immunisation schedule (as part of the 6-in-1 vaccine) and to adults >65 years old.
- Haemophilus influenzae type b (Hib) vaccine – given in early childhood to prevent Hib-related meningitis.
Vaccination is also offered to people with hyposplenism (where the spleen doesn’t work as well as it should e.g., in coeliac disease) or asplenia (those who do not have a functioning spleen). The spleen plays a crucial role in fighting certain bacterial infections, particularly encapsulated bacteria like Neisseria meningitidis, Streptococcus pneumoniae, and Haemophilus influenzae. Because these individuals are at much higher risk of severe meningococcal disease, they are routinely offered MenB and MenACWY vaccines, as well as pneumococcal and Hib vaccines, to provide protection against multiple strains.
Studies show that meningitis vaccines are highly effective at preventing disease. Since the introduction of the MenB vaccine in 2015, there has been a 75% reduction in MenB infections in vaccinated groups.
It’s important to note though that the MenB vaccine protects individuals from developing serious disease, but it does not prevent them from carrying or transmitting the bacteria to others. This is one reason why, during outbreaks like the Kent 2026 MenB outbreak, antibiotic prophylaxis is also an essential part of the public health response, alongside vaccination.
There is a lot of misinformation circling on the internet at the moment, particularly in regard to vaccines and vaccine safety. If you haven’t already, our article “10 Common Vaccine Myths Debunked: Essential Facts Every Parent Should Know” helps to confront some of that misinformation. You can read this article here.
Meningitis prevention
Preventing meningitis relies on vaccination, hygiene, and early intervention:
- Vaccination protects children, teenagers, and high-risk groups against meningococcal, pneumococcal, and Hib meningitis.
- Good hygiene helps limit transmission: good hand hygiene, wearing a mask, avoiding sharing drinks, utensils, or cigarettes, and minimising close contact in crowded settings all help.
- Contact tracing, and subsequent antibiotic prophylaxis may be offered to close contacts during outbreaks. Public health authorities identify and inform people who may have been exposed, offering antibiotics to reduce the risk of further spread.
- Early recognition of symptoms and prompt medical care can prevent severe complications and help stop transmission.
In summary
Meningitis is a potentially life-threatening condition that requires early recognition and prompt medical treatment. Vaccination remains the most effective way to prevent meningococcal and other forms of meningitis, especially in children, teenagers, and high-risk groups. Good hygiene, awareness of early symptoms, and timely antibiotic prophylaxis during outbreaks are also critical in controlling the spread of disease.
For students and young people, it is particularly important to ensure you are up to date with recommended vaccines, to be aware of the early signs of meningitis, and to seek medical care immediately if symptoms develop. By staying informed and taking preventive measures, you can protect yourself and your community from serious infection.
Would you feel confident seeking help if you noticed early signs of meningitis in yourself or a friend? Do you think universities are doing enough to protect students during outbreaks like this? If you’re a student, how has the MenB outbreak affected you?
I’d love to hear from you! Please leave a comment down below.

Leave a comment