
Today marks the start of a 6-day walkout by resident doctors, formerly “junior doctors”, across England. The dispute between resident doctors and the government has been ongoing since 2023, with multiple rounds of strike action already behind us.
Much of the public conversation focuses narrowly on pay, though this focus obscures the far more complex reality. At its heart, this is a dispute about the future of the NHS workforce — how we train doctors, how we retain them, and whether the system can sustain itself in the years ahead.
With tensions rising between the British Medical Association (BMA) and the government, and no clear resolution in sight, it’s time to look beyond the headlines.
Contents
- The speciality training bottleneck
- Why are we training new doctors?
- The impact of the UK medical prioritisation rule
- How does a lack of speciality training posts affect us all?
- Doctors outside of training
- A shortage of training posts, but also a shortage of jobs
- A brief note on pay, and the cruel irony of RPI/CPI
- In summary: Why this matters now
The speciality training bottleneck
Public debate has largely centred the strikes around pay. But according to the BMA, the real issue runs far deeper. Beneath the headlines lies a growing workforce and training crisis that is making it increasingly difficult for doctors to progress in their careers — threatening the long‑term sustainability of the NHS itself.

Applications are rising, but training posts are not
Specialty training posts are essential for doctors to progress from their initial foundation training — the first two years after medical school — into fully qualified specialist roles such as surgeons, psychiatrists, or General Practitioners (GPs).
This year, nearly 50,000 doctors applied for speciality training — the highest number on record.
But the number of training posts has barely changed.
Graph 1 (NHS England data) shows that over the past five recruitment cycles, applicants have risen sharply while training posts have remained almost static. The NHS is producing and attracting more doctors at the end of foundation year 2 than it has the capacity for in speciality training.
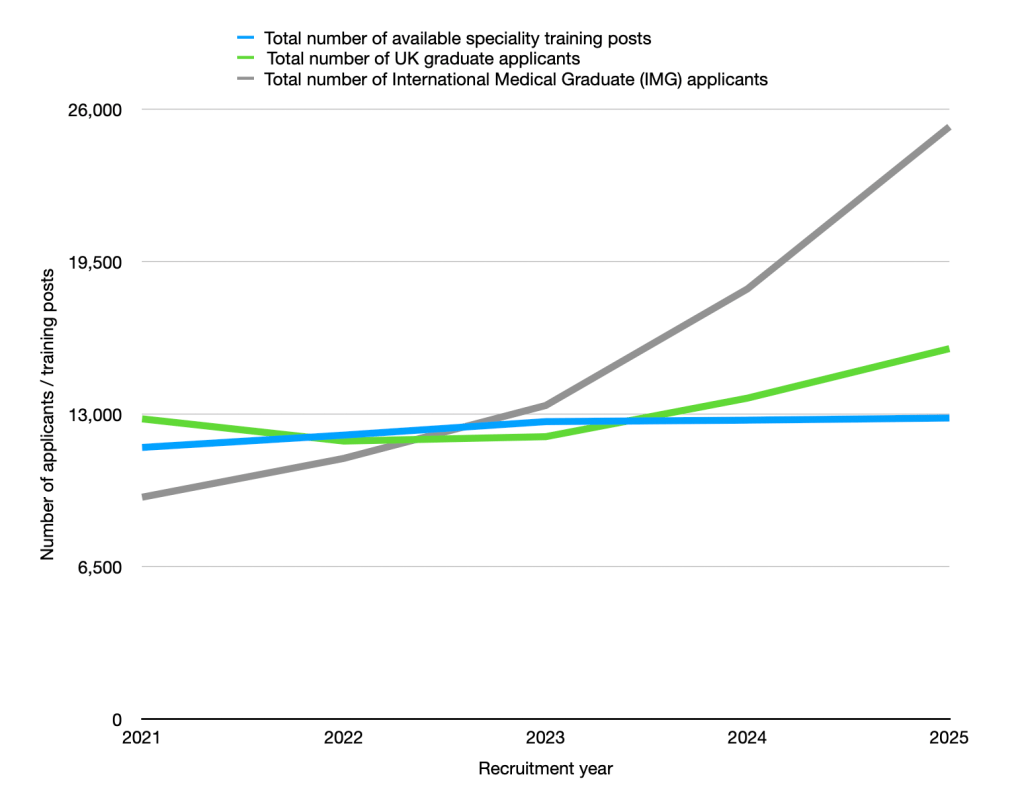
Graph 1 also shows a steep rise in International Medical Graduates (IMGs). The NHS relies heavily on IMGs to staff services — yet training posts have not expanded to match this demand.
Why are we training new doctors?
The UK has long had fewer doctors per capita than many comparable healthcare systems. According to OECD* data, the UK has around 3.37 doctors per 1,000 people in 2023, placing it near the bottom among high-income countries. For comparison:
- Austria: 5.51
- Italy: 5.35
- Germany: 4.66
- Spain: 4.39
- Australia: 4.2
- Average across all OECD countries: 3.9
A consistently low doctor-to-population ratio means the NHS has less clinical capacity to meet rising demand. This doesn’t mean that more doctors automatically produce shorter waiting times — waiting lists depend on many factors, including hospital capacity, diagnostics, social care, and funding. But the NHS is operating with fewer doctors relative to its population than comparable systems, and this contributes to the pressure patients and staff experience.
Crucially, demand is rising faster than the workforce. The NHS HR & OD report highlights that demand is being driven by “an ageing population with increasingly complex healthcare needs”. People are living longer, but with more long‑term conditions, and older adults use significantly more healthcare than younger age groups. This demographic shift means the NHS needs a larger medical workforce not just to see more patients, but to manage more complex, chronic, and resource‑intensive conditions.
The NHS Long Term Workforce Plan acknowledges this shortfall and sets out an ambitious goal: to grow the domestic medical workforce significantly over the next decade.
*Organisation for Economic Co-operation and Development (OECD): an international forum of 38 mostly development nations that aims to ‘build better policies for better lives‘.
How many more doctors does the UK actually need?
To meet the OECD average of 3.9 doctors per 1,000 people, it is estimated that the UK needs an extra 40,000 doctors. That figure is enormous — and it reflects a structural gap that has built up over decades.
The expansion of medical school places
At first glance, expanding medical school places seems like an obvious solution to the NHS workforce crisis.
Between 2018 and 2020, medical school places have already increased by around 25%, rising to roughly 7,500 places per year.
The NHS long‑term plan goes further: the government aims to double medical school places to 15,000 a year by the early 2030s.
The goal is clear — train more doctors at home rather than relying heavily on international recruitment. But expanding medical schools without expanding postgraduate training capacity creates a new problem; if the number of medical graduates rises faster than the number of training posts, the bottleneck simply moves further down the system.
The impact of the UK medical prioritisation rule
Over the past few years, competition for specialty training posts has intensified sharply — and one of the biggest drivers has been the rapid rise in IMGs applying to work and train in the UK. This surge followed immigration policy changes in 2020, which removed previous barriers and made it far easier for overseas doctors to enter NHS training pathways.
International doctors are — and always have been — essential to the NHS. Today, around 42% of doctors practising in the UK qualified abroad, and without them, many services would not function. But the sudden increase in IMG applications has collided with two other trends:
- domestic medical school expansion
- stagnant specialty training posts
The result is a system where more doctors than ever are competing for the same number of training places.
The Medical Training (Prioritisation) Act 2026
In response to growing concern about training bottlenecks, the government introduced the Medical Training (Prioritisation) Act 2026, led by Wes Streeting. The Act gives priority for specialty training posts to:
- UK medical graduates
- doctors with “significant NHS experience”
Although what constitutes “significant NHS experience” is yet to be defined, early indications suggest that two years of NHS work may qualify.
The BMA has cautiously welcomed the legislation as a positive first step. It addresses long‑standing concerns about competition for training places, particularly the rapid rise in IMG applicants. But the union is clear: prioritisation does not solve the underlying problem.
If the number of training posts stays the same, the system will still be overwhelmed — just with a different group of doctors at the front of the queue.
What the BMA’s modelling shows
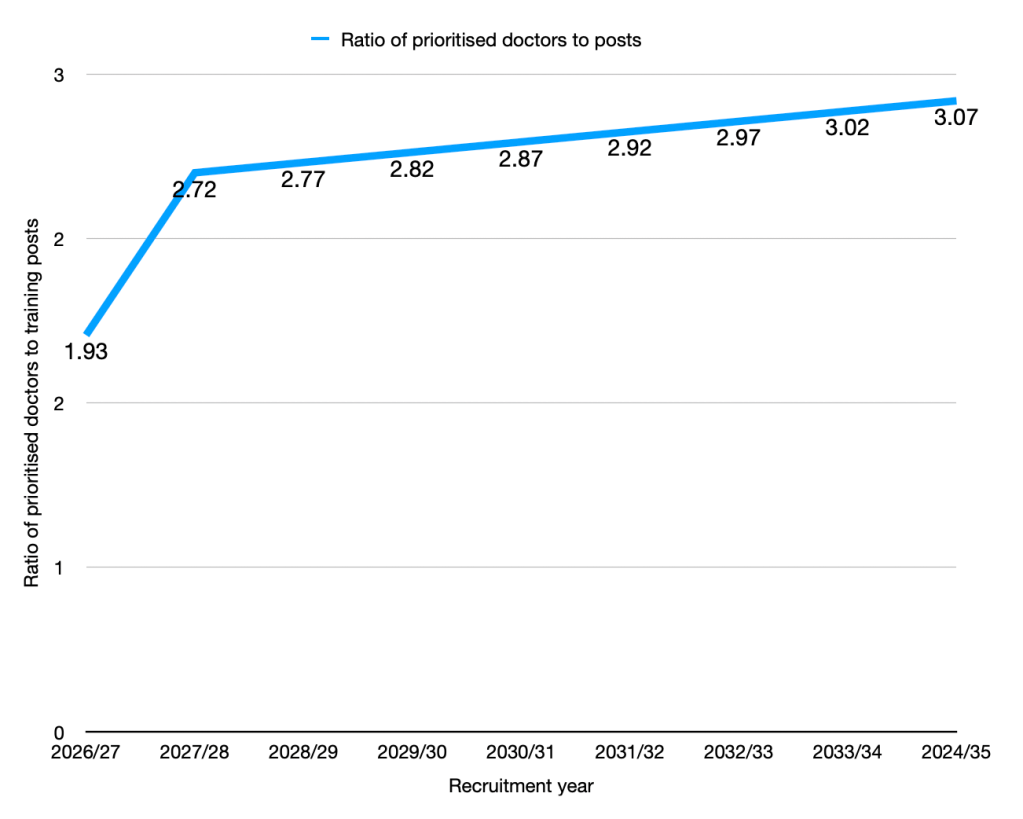
To understand how prioritisation might work in practice, the BMA modelled future competition for speciality training posts. In this context, “prioritised doctors” refers to UK medical graduates and IMGs who have worked in the NHS for two or more years.
The modelling assumes training capacity expands by:
- 1,000 additional posts in 2026/27, rising to
- 1,500 per year from 2027/28, broadly in line with current government proposals.
This expansion slows the rate at which competition worsens — but it does not reverse it. The number of doctors eligible for training continues to grow faster than the number of posts being created, meaning the bottleneck persists even under optimistic assumptions.
How does a lack of speciality training posts affect us all?
It’s easy to assume that a shortage of specialty training posts affects only resident doctors. In reality, the consequences ripple across the entire NHS. When thousands of doctors cannot progress into the specialist roles the health service depends on, the impact is felt in every clinic, every hospital, and ultimately by every patient.
1) Fewer specialists, longer waits
Specialty training is the route to becoming a consultant, GP, psychiatrist, surgeon, or physician. When doctors can’t progress, fewer specialists qualify, and the NHS cannot replace those who retire or leave. This directly feeds into the long waits patients already face for GP appointments, outpatient clinics, surgery, and mental health care.
2) The NHS loses doctors it cannot afford to lose
When doctors repeatedly fail to secure training posts, many leave the NHS or move abroad for clearer career pathways.
The health service — funded largely by taxpayer contributions — invested around £230,000 per medical student in 2017 (about £311,000 in today’s terms) only to lose them because it cannot offer progression.
It is demoralising for doctors and economically wasteful for the NHS.
3) It undermines the future consultant and GP workforce
The government has set ambitious targets for expanding the NHS workforce. But without expanding training posts, these targets become mathematically impossible.
You cannot increase the number of consultants or GPs if you do not increase the number of training places required to produce them.
The bottleneck today becomes the workforce shortage of tomorrow.
4) Rising demand, shrinking capacity, and growing pressure on existing staff
Demand for NHS care is increasing year on year. For many patients, it is now harder than ever to see a doctor — whether that’s a GP appointment, a specialist clinic, or urgent care.
When fewer doctors progress into training:
- existing staff are stretched thinner, covering more patients with the same or fewer colleagues
- senior doctors carry heavier clinical and supervisory loads, supporting larger numbers of junior staff who cannot progress.
- rota gaps can widen, making services harder to staff safely.
This can then create a cycle of burnout, sickness absence, and further workforce loss.
5) Reduced continuity of care
As Locally Employed Doctor (LED) posts become harder to secure, more are forced into short‑term locum work. This means:
- patients see different doctors from week to week
- the NHS pays more, because locum rates are typically higher
- more uncertainty for doctors, as locum work is not guaranteed
A system that relies on short‑term staffing is more expensive and delivers less consistent care.
Doctors outside of training
One of the least discussed consequences of the training bottleneck is the growing number of doctors working in non-training roles, often called Locally Employed Doctors (LEDs) or clinical fellows.
These doctors provide essential clinical service within hospitals, but they sit outside the structured national training programmes. As a result, they face several challenges:
- limited access to structured teaching
- fewer opportunities for career and pay progression
- uncertainty about long-term career pathways
Some eventually enter training after several attempts, though doing so may require dropping back to a level below their actual experience. Others remain in service posts for years with limited opportunity to negotiate pay increases, despite having the skills and experience to progress further. The NHS relies heavily on this workforce — but the career structure for these doctors remains poorly defined, leaving many doctors stuck in roles that neither recognise nor develop their full potential.
A shortage of training posts, but also a shortage of jobs
This is the paradox few people talk about.
Even in specialties with severe shortages, there are not enough jobs at the end of training. The bottleneck doesn’t just exist at the entry point — it exists at every level.
General practice is a striking example. Despite constant political rhetoric about GP shortages, GP unemployment is now widespread. Many GP trainees — myself included — face the real possibility of completing training only to find no substantive job available in the UK.
The system is producing more doctors at every stage — medical school, foundation years, specialty training — without creating the jobs required to employ them.
A brief note on pay, and the cruel irony of RPI/CPI
Pay has understandably become the most visible part of the current dispute. Resident doctors argue that their salaries have fallen significantly in real terms over the past decade, while the government says it has already offered one of the largest public-sector pay increases in recent years.
The debate itself is complicated by the fact that different measures of inflation are used. Doctors typically compare their pay to the Retail Price Index (RPI), which includes housing costs and student loan interest. The government instead uses Consumer Price Index (CPI), a lower measure of inflation.
This creates an unusual situation for many workers across the public sector: the government uses RPI to calculate student loan interest, which tends to run higher, while wage settlements are usually assessed using CPI. It is, indeed, a cruel irony.
It’s also important to acknowledge why public opinion can feel divided. Pay erosion has affected the entire public sector, not just doctors. Nurses, teachers, paramedics, civil servants, and many others have all seen their wages fall behind the cost of living over the past decade. Against that backdrop, the call for full pay restoration can feel, to some, like one group asking for something others have not received.
Because the details of the pay dispute are complex, I’ve covered them separately in my previous article Are Doctors Underpaid in 2025? The Real Numbers Behind the NHS Pay Dispute.
In summary: Why this matters now
In recent weeks, the Prime Minister has spoken about the financial cost of strike action and the pressure it places on the NHS. But the government’s decision to withdraw the 1,000 additional specialty training posts after strikes were announced illustrates a deeper problem — one that goes far beyond any single dispute.
Specialty training posts are not a political lever. They are the mechanism by which the NHS produces its future consultants, GPs, psychiatrists, surgeons, and physicians. Removing them — even temporarily — does not just affect resident doctors. It affects patients, services, and the long‑term sustainability of the health system.
Ultimately, doctors are asking for a system in which they can train, progress, and stay. A system that values the public investment made in them. A system that can meet the needs of patients not just today, but in ten years’ time.
Editor’s note: This is a complex and often emotional topic. My aim here is to inform, not inflame – and to encourage fair, open discussion. If you have thoughts or experiences to share, I’d love to hear them – but please keep any comments respectful of differing views.

Leave a comment