
By Lisa Banirian
Just as every structure needs a strong foundation, our bodies are supported by the spine.
The spinal column consists of five regions and a total of 33 vertebrae, some of which are fused by adulthood. The spine works in conjunction with muscles, tendons, ligaments, and nerves that support movement and protect the spinal cord, which carries information from the brain to the rest of the body. This framework allows the body to achieve mobility, stability, and flexibility.
Each region — cervical, thoracic, lumbar, sacral, coccygeal — has distinct anatomical features and functions essential for our bodies’ overall support and movement. When viewed from behind, a healthy spine appears straight with vertebrae stacked like building blocks to keep us upright and balanced. From the side, it forms a natural ‘S’-shaped curve that helps maintain an upright posture and supports body weight.
Adolescence is a time of rapid growth accompanied by many physical changes. At the onset of puberty, certain developmental conditions can emerge. Among these is scoliosis, a condition affecting the spine’s natural alignment. Unlike healthy spinal anatomy, scoliosis is characterised by an abnormal lateral curvature of the spine accompanied by structural asymmetries.
This article explores diagnosis, treatment options, and ongoing management, while emphasising the importance of community awareness and advocacy. By connecting readers with trusted sources and initiatives, it encourages proactive spinal health among youth.
Contents
- Defining Adolescent Idiopathic Scoliosis
- Recognising the signs
- Scoliosis signs checklist
- Diagnosis and treatment
- Psychological impact of AIS
- The power of awareness and advocacy
- Getting involved
- Celebrating scoliosis awareness month – June
DISCLAIMER: While I am a practising doctor, the information on this site is for educational purposes only. It does not take into account your personal circumstances, which can significantly affect medical decision-making and treatment. This content therefore does not constitute medical advice, and should not be relied upon for diagnosis or treatment. Always consult a qualified healthcare provider regarding any health concerns.
This article was written by a guest writer, and published on the 29/06/2026 using up-to-date sources at that time. Please be aware that medical information and guidelines change often.
Defining Adolescent Idiopathic Scoliosis
The British Scoliosis Society defines scoliosis as a spinal deformity characterised by a three-dimensional lateral curvature of the spine shaped as an ’S’ or a ‘C’. While several types exist, approximately 80% of cases are termed idiopathic, meaning the cause is unknown. Among these, adolescent idiopathic scoliosis (AIS) is the most common type, typically developing in youth between the ages of 10 and 18. Understanding what scoliosis is — and recognising it early — plays a critical role in timely treatment and optimising outcomes.
Recognising the signs
AIS most often develops in healthy children at the onset of puberty, around the age of 10, during which rapid spinal growth can promote curve progression. Detecting visible changes in posture or spinal alignment is essential. In the U.S., the Scoliosis Research Society recommends screening girls ages 10 and 12, and boys at 12 or 13. By contrast, the UK National Screening Committee (NSC) does not recommend early screening due to the lack of supporting evidence.
Scoliosis signs checklist
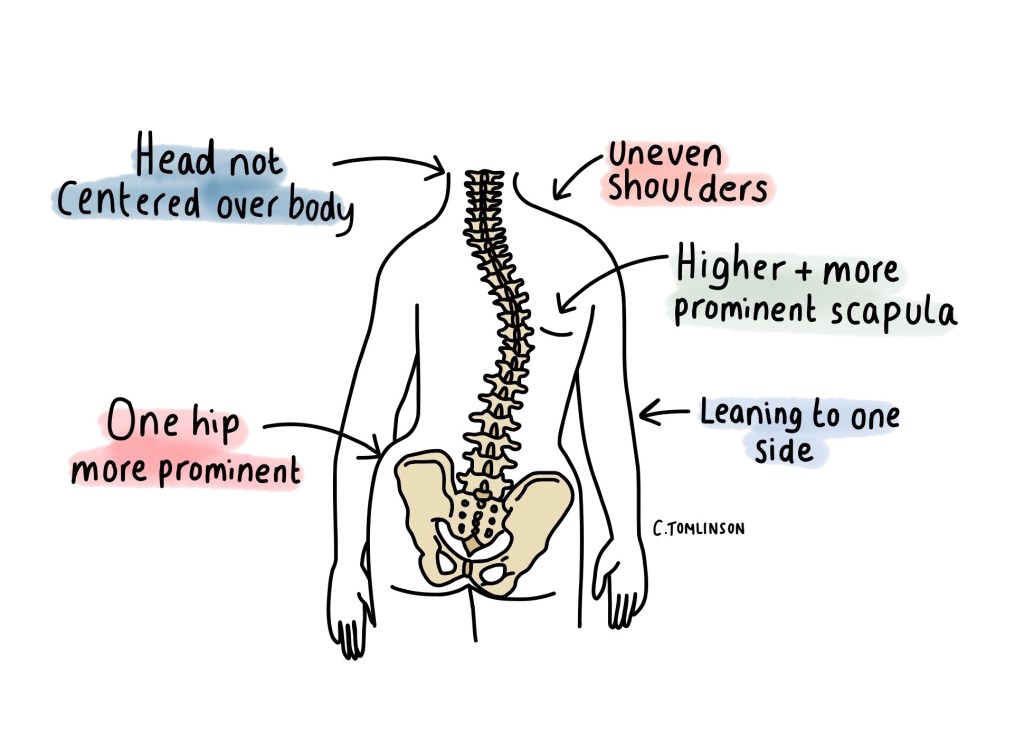
Below is a checklist of the most common signs of scoliosis. These observations are more effective when standing in front of a mirror or with the help of someone else:
- Rib hump – when bending forward, one side of the ribs appears higher.
- Uneven shoulders – one shoulder sits higher than the other.
- Shoulder blade difference – one shoulder blade (scapula) is more prominent.
- Uneven waist or hips – one side of the waist or hip looks higher or flatter.
- Head alignment – the head is not centered over the body.
- Leaning on one side – the body tilts to one side.
The UK National Health Service (NHS) recommends consulting a general practitioner (GP) if these signs are noticed and scoliosis is suspected. If scoliosis is present, a referral is made to an orthopaedic spine specialist for further evaluation and treatment options.
Diagnosis and treatment
Diagnosis begins with a postural examination of the back during which the patient is assessed for body symmetry. A healthcare provider then performs the Adams Forward Bend Test, during which the patient bends forward at the waist to observe for spinal rotation or rib prominence. This allows for measuring the amount of trunk rotation using a tool called a scoliometer.
If scoliosis is suspected, an X-ray will be performed to confirm and measure the degree of spinal curvature, known as the Cobb angle. Generally, scoliosis is defined as a spinal curvature with a Cobb angle of 10 degrees or more. Additional radiographic imaging may be performed to further assess the overall condition. The UK Scoliosis Support & Research and NHS follow treatment guidelines based on curve severity that help determine the best course of management.
The benefits of timely intervention
Although patients with scoliosis can live a normal, active life without any significant pain or other health problems, timely intervention can significantly improve long-term outcomes. Untreated scoliosis in young children can impair lung development and respiratory function in severe cases. It can also go on to affect spinal mechanics, causing nerve compression and back pain.
Observation
Patients with curves less than 20° or those with skeletal maturity (who have stopped growing) may be evaluated by the clinical team every 6-12 months for reassessment and X-ray. More frequent consultations might be necessary if the child is growing quickly. The goal is to track curve changes and to decide when treatment should begin.
Bracing
Children with curves between 20° and 40° who are still growing may be recommended for bracing treatment. A brace is a non-invasive, conservative option that aims to halt the curve progression until the patient has stopped growing. Certain factors contribute to the effectiveness of bracing treatment, but daily wear time is the most essential.
There are three main types of braces to treat scoliosis: cast, for infantile idiopathic scoliosis, rigid braces with 3-point pressure treatment principle, and non-rigid dynamic braces that use dynamic forces to stabilise the curve. The choice of brace depends on the treating physician and the patient’s needs. Prompt detection and diagnosis are key to initiating timely bracing and improving treatment outcomes.
Surgery
Posterior spinal fusion may be recommended for patients with curves of 45° or greater, and/or who are at risk of continued worsening even after they have reached their growth target. Spinal fusion remains the most established and widely used procedure to date. This surgery uses metal rods, screws, hooks or wires, along with bits of bone taken from elsewhere in the body to correct the spinal vertebrae’s position. This procedure fuses the vertebrae in place, ceasing the curve’s progression.
For younger children under 10 years old, a different approach is taken. Temporary growing rods are used to correct the curve while allowing their spine to keep growing. Through a minor incision in the back or using magnets, these rods are periodically lengthened to manage the curve until the child reaches skeletal maturity. Afterwards, the rods may be removed and a final surgery is performed to fuse the spine permanently. Scoliosis surgery stabilises the spine in a corrected position, improving spinal alignment and posture.
Complementary Approaches
The goal in early treatment of scoliosis is to halt curve progression, ultimately avoiding surgery. Scoliosis Support & Research defines complementary therapies as treatments that work alongside primary interventions, such as bracing. Therapies such as physiotherapy, especially individualised exercises, can greatly reduce back pain, relax muscles, and improve mobility. Massage therapy can relieve muscle tension and promote relaxation. Exercises such as yoga or Pilates can help strengthen core muscles, improve posture, and support breathing. The treating physician can help direct patients to the appropriate complementary therapy.
Psychological impact of AIS
Scoliosis can have a significant psychosocial impact on a child or teenager’s life. Diagnosis can lead to uncertainties of the condition and its long-term implications, contributing to stress, anxiety, and depression. Physical changes due to scoliosis may negatively affect body image and self-esteem, and introduce social and intimacy restrictions. In addition, the physical restrictions and visible appearance of the brace can play a significant role in the patient’s mental health and well-being, leading to feelings of embarrassment and social isolation. Given these circumstances, scoliosis peer-support groups are essential to patients and their families to help them navigate their treatment journey with supportive and trusted care. The UK Scoliosis Support & Research has a helpline and online peer-support groups led by qualified counsellors.
The power of awareness and advocacy
Advocacy plays a vital role in improving outcomes for children with scoliosis. Sharing clear, accurate, accessible information ensures early referrals and timely treatment. A study from the SickKids Hospital in Toronto found that 58% of scoliosis cases were first noticed by a non-medical person — most often by family members or the children themselves.
This underscores the impact of community awareness. When parents, teachers, sports coaches, family members, and peers are informed, they can help identify scoliosis early and encourage proper medical evaluation.
Getting involved
Friends, families, community members, school personnel, community sports organisations, healthcare professionals, and all allied health professionals are encouraged to take action in this initiative to raise awareness of Adolescent Idiopathic Scoliosis within their communities. There are various advocacy groups across the world that engage the public and provide community outreach programs to disseminate reliable medical information on AIS awareness, diagnosis, and treatment. Advocacy has a direct, positive impact by encouraging and supporting youth to actively participate in their health journey and make informed decisions.
By joining your local advocacy group or simply being informed about AIS, we each have the power to foster a culture of mutual care. Here are some of the ways being part of a support group can benefit patients and families:
- Empowers patients and families
- Provides hope and encouragement
- Builds a sense of community and belonging
- Promotes peer-to-peer dialogue and friendship
- Reduces isolation and anxiety
Celebrating scoliosis awareness month
Each June marks Scoliosis Awareness Month — a time to promote early detection, education, and community support for adolescents affected by scoliosis. It’s an opportunity to raise visibility, advocate for standardised screening, and celebrate the resilience of those living with scoliosis.
Join the movement this June by connecting with these trusted organisations and many more in your local communities:
- UK Scoliosis Support & Research
- UK NSC
- UK NHS
- British Scoliosis Society
- Eurospine
- Scoliosis Research Society
By staying informed, sharing knowledge, and supporting early screening, we can help more children stand tall — and strong — against scoliosis.

Lisa Banirian is a freelance Montreal-based health and advocacy writer focused on scoliosis. Diagnosed at age eight, she combines lived experience with a healthcare background to promote early detection, education, and support, empowering readers to take an informed, proactive role in their health. She currently works as a medical representative.
She can be reached at lisabanirian@gmail.com or www.linkedin.com/in/lisa-banirian

Leave a comment