
By Josette Pelatan, PhD
Editor’s note: This article is a first-person opinion and lived-experience piece by a guest writer. The views expressed are those of the author and reflect her individual healthcare journey. Personal experiences with illness, diagnosis, and treatment can vary significantly, and this article is not intended to provide medical advice, replace professional clinical assessment, or generalise all patient or clinician experiences.
I never imagined that the scientific training I trusted would one day abandon me — or that I would, by necessity, become my own diagnostician. For more than a decade, my body unraveled in ways that medicine repeatedly failed to explain. What began as pervasive fatigue quickly escalated into a constellation of neurologic and systemic symptoms that intensified in frequency, duration, and severity.
Weeks of profound weakness left my knees giving way beneath me; episodes that once lasted minutes stretched into hours and then days. Cognitive disturbances left me “drunk in my own head,” with clumsiness that erased my confidence in walking and thinking. I lost my balance, and vision occasionally blurred or dimmed altogether. I endured tremors in my hands, eye and toe twitches, frightening neurologic episodes, and physical symptoms severe enough to repeatedly disrupt daily life, even with only the slightest stressor.

Despite mounting evidence of neurologic and immunologic dysfunction — swollen lymph nodes after minimal exertion, repeated emergency visits, and seizure-like episodes — the prevailing diagnosis throughout my medical journey in the United States was psychosomatic: a mental health crisis. While psychological distress can affect physical health, in my case this explanation did not fully account for the progression or severity of what I was experiencing; at thirty-something, with symptoms stacking upon one another, my brain and body felt increasingly alien.
It was profoundly frustrating and, at times, devastating. When the U.S. health system reached the limit of its willingness to investigate, I made a choice that would change my life: I became my own researcher.
Becoming a patient-scientist
I pursued medical certifications, immersed myself in clinical literature, and allowed my lived experience to guide scientific inquiry. In 2022, I crossed the border into Mexico with a single goal: to find answers I could not access at home. I successfully petitioned for admission to a PhD program in Interdisciplinary Health Sciences at the University of Texas at El Paso. There, I championed the university’s first auto-ethnographic dissertation, using my own body, medical records, and lived experience as data. I graduated with a deep appreciation for both patient narrative and academic rigour.
It was through this work that I finally received a definitive diagnosis: relapsing myelin oligodendrocyte glycoprotein antibody–associated disease (MOGAD) — a rare, often misunderstood autoimmune demyelinating disorder of the central nervous system.
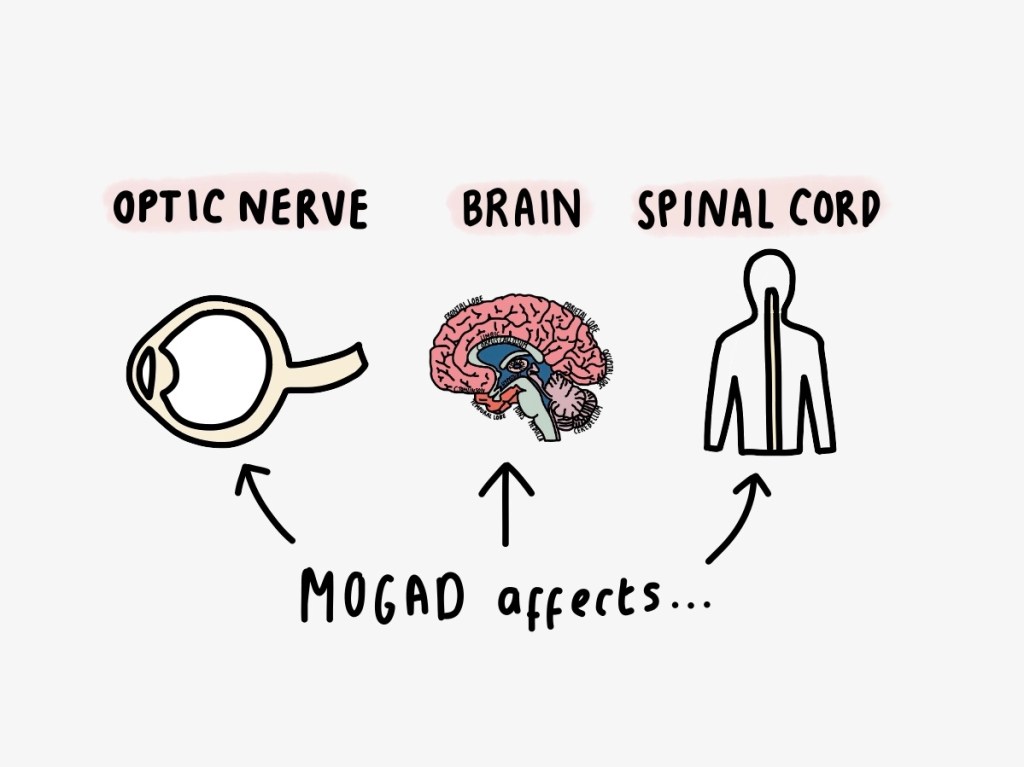
MOGAD can present with optic neuritis, myelitis, encephalopathy, and brainstem symptoms, and patients frequently experience relapses that worsen over time. What makes MOGAD clinically challenging is not only its rarity but its heterogeneous symptom profile: fatigue, blurred vision, tremors, cognitive impairment, and balance disruption — exactly the experiences that dominated my decade of unexplained illness. Studies indicate that many patients with MOGAD endure relapsing courses with cumulative disability when the disease is unrecognised. You can read more about MOGAD here.
Yet what quantitative studies alone cannot capture is the qualitative reality of living in a body that medicine repeatedly tells you is “normal” when you know, with every fibre of your being, that it is not.
Personal narratives are not anomalies; they are essential context. Stories of incremental losses, symptoms dismissed as anxiety, and physical events misattributed to psychological causes help bridge the space between lab values and human experience, reminding us that science without empathy fails at the bedside.
Post-traumatic growth: from survival to thriving
Amid this prolonged uncertainty and suffering, I discovered a concept that would reshape my understanding of illness: Post-Traumatic Growth (PTG). Coined by psychologists Richard Tedeschi and Lawrence Calhoun, PTG refers to the positive psychological change experienced as a result of adversity.
Unlike resilience, which emphasises bouncing back, PTG emphasises transformative growth — finding meaning, renewed purpose, and personal strength from experiences that challenge one’s assumptions about life and the self.
Becoming my own expert forced me to confront both the fragility of my body and the limitations of a system I had once trusted implicitly. Yet through this struggle, I developed a profound sense of agency.
Learning immunology, reading pathology reports, and decoding MRI scans were no longer simply acts of survival — they became exercises in reclaiming control. Each discovery about my disease, no matter how incremental, was a step toward empowerment.
This transformation was neither immediate nor linear. It required deep self-reflection, the capacity to forgive — not only the medical system, but my own body and the life I had lost— and the courage to envision a life beyond the constraints of illness. Forgiveness, in this context, was not about erasing harm; it was about freeing my own mind to engage fully with the present and future.
Forgiveness in the midst of misdiagnosis
Medical dismissal is often internalised, leaving patients doubting their own perceptions. For years, I oscillated between anger and despair. The PTG framework helped me reframe these emotions: I could acknowledge the failures of the system without allowing them to define my worth or dictate the trajectory of my life. Forgiveness became an act of self-liberation. By releasing the hold of resentment, I could focus energy on learning, advocacy, and rebuilding my confidence.
The journey toward forgiveness also extended to my own body. Chronic illness can create a sense of betrayal; we feel trapped in a vessel that undermines our intentions. Through PTG, I learned to view my body not as an enemy but as a partner that had endured profound stress, requiring care, patience, and respect. Recognising its resilience, even in the face of disease, became a source of gratitude and motivation.
Purpose through patient expertise
Being forced into self-expertise revealed a broader purpose: the ability to translate lived experience into meaningful contributions to science, advocacy, and education.
My research, grounded in auto-ethnography, illustrated how patients’ narratives can complement clinical data, offering insights into disease progression, symptom heterogeneity, and psychosocial impact. By sharing my story, I hope to illuminate the invisible struggles of chronic illness and encourage a more empathetic, patient-centred approach to care.
PTG emphasises that meaning-making is central to growth. For me, this meaning emerged in multiple dimensions: teaching other patients how to advocate for themselves, contributing to scientific understanding of MOGAD, and bridging gaps between patient experience and clinical practice. I no longer saw my decade-long journey as “lost time,” but as preparation for this new chapter — a period of intensive learning, self-discovery, and purpose-driven action.
Systemic lessons: listening, validating, evolving
My story also underscores a systemic problem: when patients’ experiences do not conform neatly to diagnostic templates, medicine too often defaults to psychosocial explanations. This is not merely an issue of individual clinician bias; it reflects structural limitations in research priorities, diagnostic algorithms, and healthcare accessibility. Patients forced to become their own experts do so because the system cannot — or will not — adapt to complexity.
Yet there is hope. Health systems that integrate patient narratives alongside biomarkers, that value longitudinal observation over episodic metrics, and that prioritise empathy alongside expertise are capable of transformative change. Research shows that narrative medicine helps improve diagnostic accuracy, patient satisfaction, and adherence to treatment plans (Charon, 2001). Listening to patients is not optional; it is central to ethical and effective practice.
Thriving beyond illness
PTG does not erase suffering. MOGAD remains a part of my life, and symptoms continue to present challenges. However, I now navigate these challenges with a sense of agency and purpose that illness alone could not have inspired. I have cultivated resilience that is both adaptive and generative, transforming adversity into knowledge, advocacy, and personal insight.
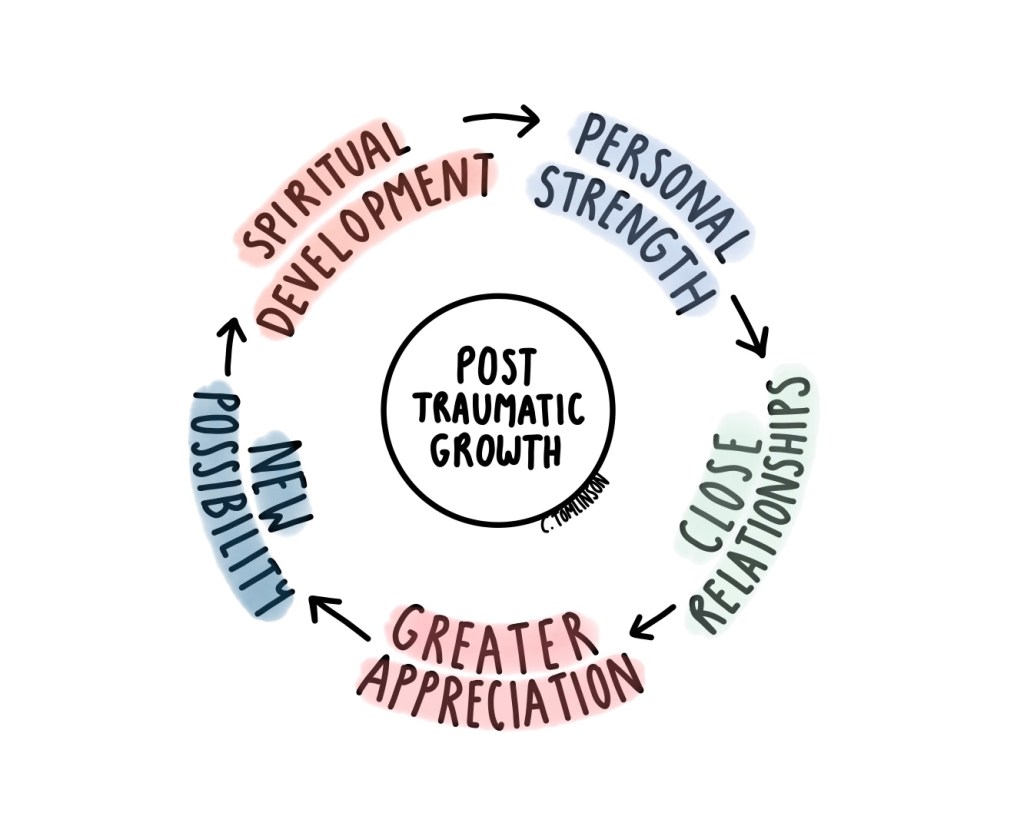
There are five domains to PTG:
- Increased personal strength – being more confident in your own ability to handle difficult, and navigating healthcare independently
- Improved relationships – connecting with those around you, including others who share chronic illness and fostering empathy
- Appreciation of life – finding gratitude in small, everyday victories, and finding value in your own life
- Spiritual or existential growth – re-evaluating priorities and embracing purpose-driven action
- New possibilities – creating pathways for research, advocacy, and education, and being open to new opportunities both professionally and personally
Through this lens, my experience is no longer defined solely by MOGAD or misdiagnosis. It is defined by the deliberate choices I made to reclaim agency, to forgive, and to discover purpose.
Moving forward
Becoming my own expert was never a path I would have chosen under ordinary circumstances. Yet it allowed me to discover inner resources I might never have otherwise cultivated: resilience in the face of uncertainty, the capacity for forgiveness, and a sense of purpose rooted in lived experience. My journey demonstrates that even in the most isolating and bewildering circumstances, patients can emerge not just as survivors but as active agents of growth and transformation.
Medicine, at its best, learns from stories. It evolves when clinicians listen, when research values lived experience alongside laboratory data, and when health systems honour suffering rather than dismiss it. Patients forced into self-expertise provide a stark reminder of what is at stake: when systems fail to adapt, the price is borne by individuals. Yet through Post-Traumatic Growth, suffering can catalyse insight, empathy, and purpose, illuminating a path from adversity to thriving.
We owe it to each other — patients, clinicians, researchers — to create spaces where no one feels compelled to become their own expert simply to be believed or cared for. Growth, forgiveness, and purpose are not abstract ideals; they are attainable outcomes when experience is honoured, expertise is democratised, and humanity guides science.
Editor’s note: Reflection on this article
Experiences of delayed diagnosis, diagnostic uncertainty, and feeling unheard are unfortunately common themes across many chronic and rare disease communities. At the same time, complex symptoms can arise from multiple overlapping physical and psychological factors, and diagnostic processes are often shaped by uncertainty rather than intentional dismissal.
Josette’s piece highlights the importance of listening closely to patients, maintaining clinical curiosity, and recognising the emotional burden of prolonged uncertainty. It also underscores the value of collaborative care, where lived experience and clinical expertise are brought into dialogue rather than positioned in opposition.
Lived experience offers a form of knowledge that complements, rather than competes with, clinical data — helping patients, clinicians, and researchers better understand the realities of navigating illness over time.
I’d love to hear your thoughts! Please leave a comment down below.
- What does “patient expertise” mean to you? Where should lived experience sit alongside clinical knowledge?
- Can adversity meaningfully reshape identity, purpose, or relationships in ways that align with post-traumatic growth? Have you seen this in your own life or work?
- How can clinicians and health systems better incorporate patient narratives into care and diagnosis?

Dr. Josette Pelatan is an interdisciplinary health scientist, patient-researcher, and storyteller whose life and work sit at the intersection of medicine, lived experience, and narrative power. Holding a PhD in Interdisciplinary Health Sciences, she is known for advancing one of the first auto-ethnographic dissertations in her program — using her own body, medical history, and lived reality as rigorous scientific data to illuminate the gaps between clinical metrics and patient experience.
Her journey into research was not purely academic; it was born from necessity. After more than a decade of escalating neurological and systemic symptoms that went unexplained and were frequently misattributed, she ultimately received a definitive diagnosis of relapsing Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD), a rare autoimmune demyelinating disorder of the central nervous system. Rather than allowing this diagnosis to define the limits of her life, Dr. Pelatan transformed it into a catalyst for purpose through the framework of Post-Traumatic Growth — reclaiming agency, cultivating forgiveness, and turning suffering into scholarship, advocacy, and action.
Today, Dr. Pelatan continues to expand her medical knowledge as an independent researcher, actively engaging with emerging clinical research to better understand the causes, treatments, and potential future therapies for relapsing MOGAD. She works to bridge the space between patient narrative and clinical science, advocating for healthcare systems that listen more deeply, investigate more curiously, and treat patients as collaborative partners in knowledge.
Beyond academia and advocacy, Dr. Pelatan is the founder and producer of JosetteXMP Productions, a storytelling platform dedicated to elevating complex human experiences that are often overlooked. She is currently fundraising for two major film projects:
- Homeless with a PhD — a documentary exploring the invisible realities of illness, displacement, and resilience among highly educated individuals navigating systemic failure.
- The Prostitute’s Daughter — a feature film examining generational trauma, dignity, and survival through an unflinching human lens.
Through both research and film, her mission is the same: to make the unseen visible, to humanize what systems overlook, and to ensure that stories—especially those born from adversity—inform how we care, how we listen, and how we build a more compassionate world.
Dr. Pelatan’s work reminds us that expertise does not belong solely to institutions. Sometimes, it is forged in hospital rooms, in long nights of uncertainty, in stacks of medical journals read by patients desperate for answers. Her life stands as an inspiration to anyone navigating chronic illness, professional setbacks, or personal upheaval: growth is possible, purpose can be reclaimed, and knowledge can be built from even the most difficult chapters of our lives.
Social Media Links:
Website: https://josettepelatan.carrd.co/
LinkedIn: https://www.linkedin.com/in/josette-pelatan-651a98261/
Facebook: https://www.facebook.com/josettepelatan
BlueSky: https://bsky.app/profile/josettexmp7.bsky.social
Instagram: https://www.instagram.com/josettepelatan/

Leave a comment